What is Complex Regional Pain Syndrome?
Complex Regional Pain Syndrome (CRPS) is a chronic pain condition most often affecting one of the limbs (arms, legs, hands, or feet).
It usually occurs following an injury or trauma to that limb. Trauma could be a Major one (e.g. limb fracture, cut wound, crush injury,.…) or Minor trivial ones (e.g. mosquito bite, ankle sprain,…).
CRPS is believed to be caused by damage to, or malfunction of, peripheral and central nervous systems.
CRPS is characterized by prolonged or excessive pain and mild or dramatic changes in skin color, temperature, and/or swelling in the affected area.
Types of CRPS:
There are two similar forms, called CRPS-I (formerly called Reflex Sympathetic Dystrophy) and CRPS-II (formerly Causalgia), with the same symptoms and treatments.
CRPS-II, is the term used for patients with confirmed nerve injuries. Individuals without confirmed nerve injury are classified as having CRPS-I. Some research has identified evidence of nerve injury in CRPS-I, so the validity of the two different forms is being investigated.
** Studies of the incidence and prevalence of the disease show that with early diagnosis, intervention and guided treatment most cases are mild and individuals can recover completely. In more severe not treated cases, individuals may not recover and may have long-term disability.
Who can get CRPS?
Anyone can get CRPS. It can strike at any age and affects both men and women, although it is much more common in women. The average age of affected individuals is about age 40. CRPS is rare in the elderly. Children do not get it before age 5 and only very rarely before age 10, but it is not uncommon in teenagers. Children and adolescents with CRPS generally have a better recovery than adults and offer a unique model for the study of chronic pain reversal. Scientists studying children with CRPS are investigating neuroplasticity and the biological processes that cause CRPS to occur, in the hopes of developing more effective therapies and accelerated recoveries for adults and children.
Symptoms:
CRPS symptoms vary in severity and duration
Pain is the key symptom, and it is usually prolonged constant and, in some people, extremely uncomfortable or severe. The pain may feel like a burning or “pins and needles” sensation, or as if someone is squeezing the affected limb. The pain may spread to include the entire arm or leg, even though the precipitating injury might have been only to a finger or toe. Pain can sometimes even travel to the opposite extremity. There is often increased sensitivity in the affected area, such that even light touch or contact is painful (called Allodynia).
People with CRPS also experience constant or intermittent Changes in temperature, skin color, and swelling of the affected limb. This is due to abnormal microcirculation caused by damage to the nerves controlling blood flow and temperature. An affected arm or leg may feel warmer or cooler compared to the opposite limb. The skin on the affected limb may change color, becoming blotchy, blue, purple, pale, or red.
Other common features of CRPS include:
- Changes in skin texture on the affected area; it may appear shiny and thin
- Abnormal sweating pattern in the affected area or surrounding areas
- Changes in nail and hair growth patterns
- Stiffness in affected joints
- Problems coordinating muscle movement, with decreased ability to move the affected body part
- Abnormal movement in the affected limb, most often fixed abnormal posture (called dystonia) but also tremors in or jerking of the affected limb.
Causes of CRPS:
Doctors aren’t sure what causes some individuals to develop CRPS while others with similar trauma do not. In more than 90 percent of cases, the condition is triggered by a clear history of trauma or injury.
The most common triggers are fractures, sprains/strains, soft tissue injury (such as burns, cuts, or bruises), limb immobilization (such as being in a cast), or surgical or medical procedures (such as Needlestick).
CRPS represents an abnormal response that magnifies the effects of the injury. In this respect it is like an allergy. Some people respond excessively to a trigger that causes no problem for other people.
Mechanisms involved in CRPS development:
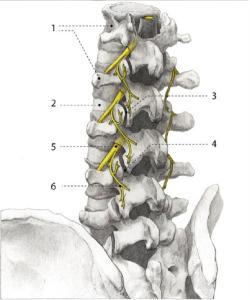
Nerves:
Peripheral nerve abnormalities found in individuals with CRPS, it usually involve the small unmyelinated and thinly myelinated nerve fibers (axons) that carry pain messages and signals to blood vessels. (Myelin is a mixture of proteins and fat-like substances that surround and insulate some nerve fibers.) Because small fibers in the nerves communicate with blood vessels, small nerve fiber injuries may trigger the many different symptoms of CRPS. Molecules secreted from the ends of hyperactive injured small nerve fibers are thought to contribute to inflammation and blood vessel abnormalities. These peripheral nerve abnormalities in turn trigger abnormal neurological function in the spinal cord and brain, leading in some cases to complex disorders of higher cortical function.
Blood Vessels
Another abnormality in CRPS involves the Blood Vessels in the affected limb, which may dilate (open wider) or leak fluid into the surrounding tissue, causing red, swollen skin. The underlying muscles and deeper tissues can become starved of oxygen and nutrients, causing muscle and joint pain and damage. At times, the blood vessels may over-constrict (clamp down), causing cold, white, or bluish skin. The dilation and constriction of small blood vessels is controlled by small nerve fiber axons as well as chemical messengers in the blood.
Immune System
CRPS also affects the Immune System. High levels of inflammatory chemicals (cytokines) have been found in the tissues of people with CRPS. These contribute to the redness, swelling, and warmth reported by many patients. CRPS is more common in individuals with other inflammatory and autoimmune conditions such as asthma.
Others: Genetics, Family History….
Limited data suggest that CRPS also may be influenced by genetics. Rare family clusters of CRPS have been reported. Familial CRPS may be more severe with earlier onset, greater dystonia, and more than one limb being affected.
Occasionally CRPS develops without any known injury. There may have been an internal injury caused by an infection, a blood vessel problem, or entrapment of the nerves, so careful examination is needed to determine the cause and treat it.
**In many cases, CRPS is the result of multiple causes that act together to produce various symptoms.
Diagnosis:
Currently there is No single diagnostic test to confirm CRPS, it is purely clinical evaluation. Diagnosis is based on the affected individual’s medical history and signs and symptoms that match the definition.
Because several other conditions can cause similar symptoms, careful examination is important and clinical correlation is key to get the right diagnosis early in the disease for treatment and intervention.
Testing also may be used to help rule out other conditions, such as arthritis syndromes, Lyme disease, generalized muscle diseases, a clotted vein, or small nerve fiber polyneuropathies (such as from diabetes), because these require different treatment. The distinguishing feature of CRPS is usually a history of earlier injury to the affected area, as most of these other conditions are not triggered by injury. Individuals without a history of injury should be carefully examined to make sure that another treatable diagnosis is not missed.
Magnetic Resonance Imaging - MRI or tri-phasic Bone Scans sometimes identify CRPS-characteristic changes in the bone metabolism. CRPS is often associated with excess bone resorption, a process in which certain cells break down the bone and release calcium into the blood.
Outcome and Prognosis:
Anecdotal evidence suggests early treatment and intervention, particularly targeted rehabilitation, is helpful in limiting the disorder and avoiding long term disability. I always tell my patients that the main concern now is how to keep your affected limb active, without loosing its functional ability. Getting the pain out of the way is crucial in order to get involved in targeted rehabilitation and recovery program.
With the early Accurate Diagnosis and the right intervention, children and adolescents with CRPS generally have a better recovery than adults and offer a unique model for the study of chronic pain reversal. Scientists studying children with CRPS are investigating neuroplasticity and the biological processes that cause CRPS to occur, in the hopes of developing more effective therapies and accelerated recoveries for adults and children.
The outcome of CRPS varies from person to person. Almost all children and teenagers have good recovery. Some individuals are left with unremitting pain and crippling, irreversible changes despite treatment.
Modalities and Roles in Treating CRPS
Treatment Goals are:
- Pain Control
- Getting engaged in aggressive Rehabilitation program to keep the limb functioning, and avoiding irreversible damage to the affected body part.
Non Interventional:
Rehabilitation Therapy. An exercise program to keep the painful limb or body part moving can improve blood flow and lessen the circulatory symptoms. Additionally, exercise can help improve the affected limb’s flexibility, strength, and function. Rehabilitating the affected limb also can help to prevent or reverse the secondary brain changes that are associated with chronic pain. Occupational therapy can help the individual learn new ways to work and perform daily tasks.
Medications. Several different classes of medication have been shown to be effective for CRPS, particularly when used early in the course of the disease. No drug is approved by the U.S. Food and Drug Administration specifically for CRPS. No single drug or combination of drugs is guaranteed to be effective in every person. Drugs to treat CRPS include:
- Non-Steroidal Anti-Inflammatory Drugs to treat moderate pain, including over-the- counter aspirin, ibuprofen, and naproxen
- Corticosteroids that treat inflammation/swelling and edema, such as prednisolone and methylprednisolone (used mostly in the early stages of CRPS)
- Nerve Membrane Stabilizers, drugs initially developed to treat seizures or depression but now shown to be effective for neuropathic pain, such as Gabapentin, Pregabalin, Amitriptyline, Nortriptyline, and Duloxetine, Botulinum toxin injections
- Opioids such as Oxycontin, Morphine, Hydrocodone, Fentanyl, and Vicodin
- N-methyl-D-aspartate (NMDA) receptor antagonists such as Dextromethorphan and Ketamine
- Others: nasal calcitonin, especially for deep bone pain, and topical local anesthetic creams and patches such as lidocaine.
All drugs or combination of drugs can have various side effects such as drowsiness, dizziness, increased heartbeat, and impaired memory. These medications are given under close monitoring by your pain or primary care physician.
Psychotherapy. CRPS and other painful and disabling conditions often are associated with profound psychological symptoms for affected individuals and their families. People with CRPS may develop depression, anxiety, or post-traumatic stress disorder, all of which heighten the perception of pain and make rehabilitation efforts more difficult. Treating these secondary conditions is important for helping people cope and recover from CRPS.
Interventional Approaches
Sympathetic Nerve Block
CRPS believed to be a Sympathetic Mediated Pain (SMP) condition, and sympathetic nerve block serves as a diagnostic / therapeutic to the problem. It involve injecting an Anesthetic next to the spine to directly block the activity of sympathetic nerves, which in turn, block the Sympathetic Mediated Pain sensation and improve blood flow to the affected limb. Pain relief and improved functionality of the affected organ following the Sympathetic Nerve Block is considered a good prognostic factor to the overall outcome of the condition.
Surgical Sympathectomy
The use of this operation that destroys some of the nerves is controversial. Some experts think it is unwarranted and makes CRPS worse; others report a favorable outcome. Sympathectomy should be used only in individuals whose pain is dramatically relieved (although temporarily) by sympathetic nerve blocks. It also can reduce excess sweating.
Spinal Cord Stimulation
Simply, the Spinal cord stimulation (SCS), consists of electrical energy producing electrodes placed in the epidural space, and connected to electrical pulse generator that transmits signals to dorsal part of the spinal cord, interrupting pain signals from reaching the brain. SCS has notable analgesic properties and is successfully in the treatment of Complex Regional Pain Syndrome. Again, the whole point is to get the pain out of the way to keep the limb fully functional, and sometime the SCS is the answer to achieve that.
Intrathecal Drug Delivery System
These devices pump pain-relieving medications directly into the fluid that bathes the spinal cord, typically opioids and local anesthetic agents such as Clonidine and Baclofen. The advantage is that pain-signaling targets in the spinal cord can be reached using doses far lower than those required for oral administration, which decreases side effects and increases drug effectiveness. Most patients will undergo a trial of about seven days before permanent implantation to ensure efficacy and pain relief.
Other possible treatments for CRPS:
- Ketamine. Investigators are using low doses of ketamine—a strong anesthetic—given intravenously for several days to either reduce substantially or eliminate the chronic pain of CRPS. In certain clinical settings, ketamine has been shown to be useful in treating pain that does not respond well to other treatments.
- Intravenous immunoglobulin (IVIG). Researchers in Great Britain reported that low-dose IVIG reduced pain intensity in a small trial of 13 patients with CRPS for 6 to 30 months who did not respond well to other treatments. Those who received IVIG had a greater decrease in pain scores than those receiving saline during the following 14 days after infusion. A larger study involving individuals with acute-phase CRPS is planned.
- Several alternative therapies have been used to treat other painful conditions. Options include behavior modification, acupuncture, relaxation techniques (such as biofeedback, progressive muscle relaxation, and guided motion therapy),



![By James Heilman, MD (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons](/assets/components/phpthumbof/cache/vcfrac3.25c355a85cb0101f004729be8d39bec3204.jpg)